Pipeline
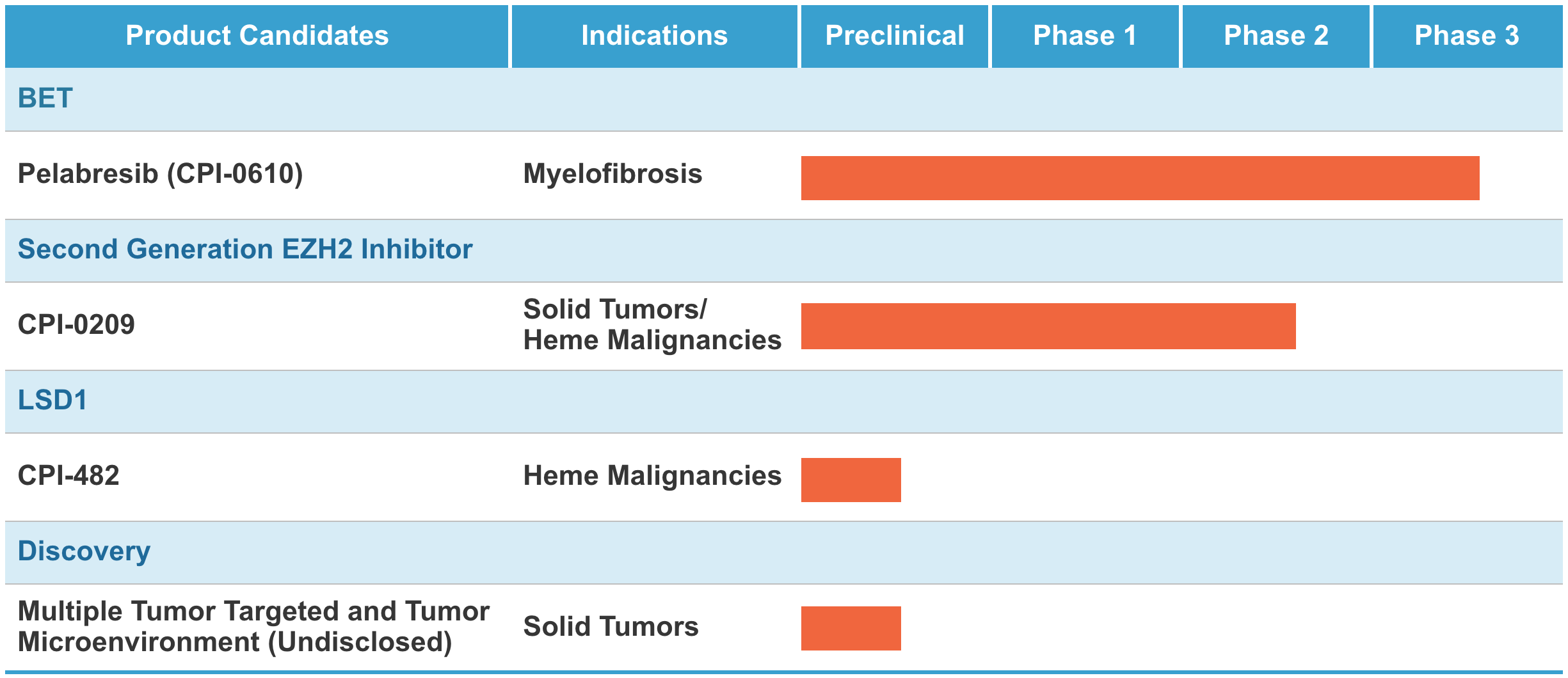
The following table summarizes key information about our most advanced programs:
BET
A Scientific Overview
Bromodomain and extra-terminal domain (BET) proteins act as epigenetic readers, transmitting the signal carried by acetylated lysine residues on histones and transcribing it into various phenotypes. Abnormal BET function has been implicated in cancer through several means, including chromosomal translocation, gene amplification, and gene overexpression whereby oncogenic and inflammatory signals are turned on in cancer cells through altered BET activity.
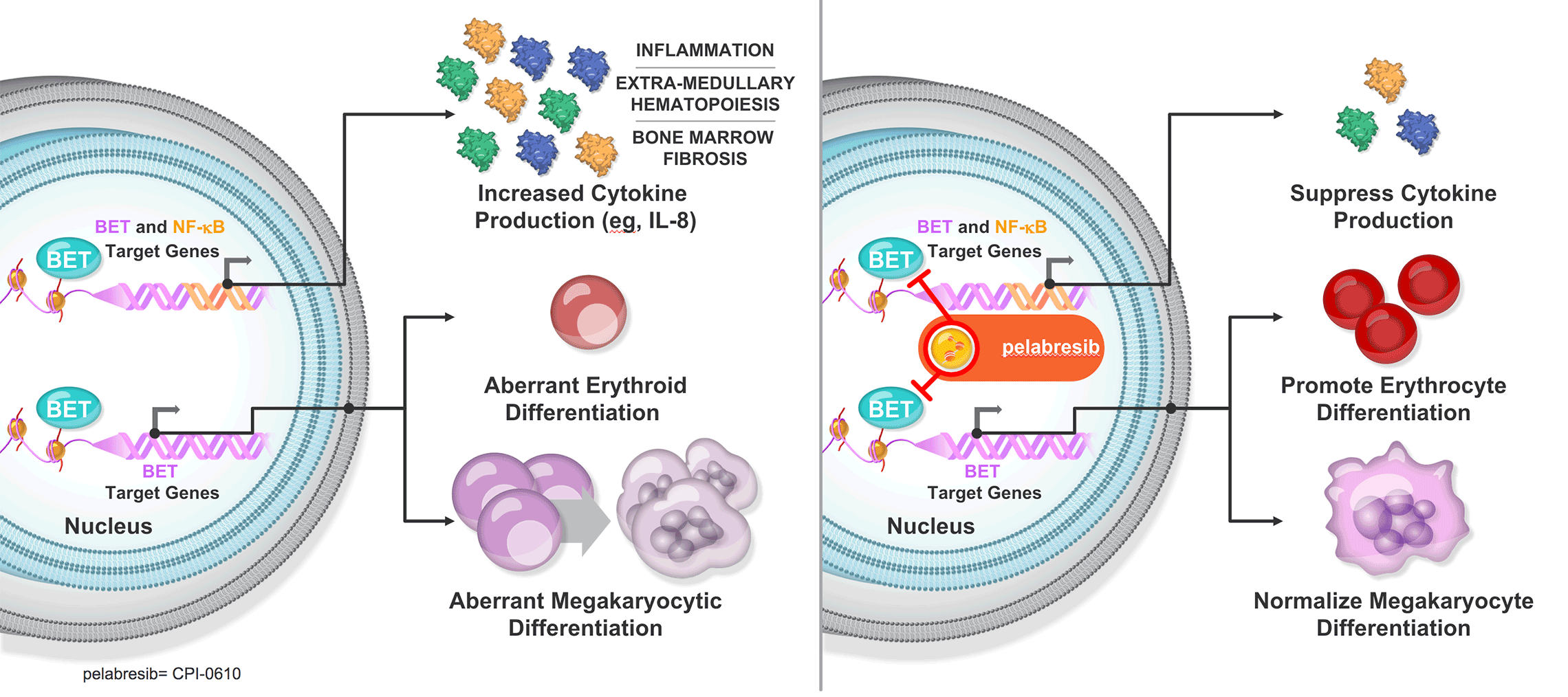
Dysregulated BET signaling is involved in a number of diseases, including myelofibrosis (MF), a progressive hematological cancer, by promoting the generation of aberrant megakaryocytes from hematopoietic stem cells. We believe that the blood cells most responsible for MF are dysfunctional megakaryocytes, which proliferate and produce inflammatory molecules, in part through elevated NF-κB target gene expression. Abnormally activated NF-κB is involved in the production of pro-inflammatory cytokines, such as interleukin-8. In addition to playing a role in megakaryocyte differentiation, BET proteins also control the expression of these NF-κB target genes. In preclinical studies in MF, animals treated with a BET inhibitor alone or in combination with ruxolitinib (a JAK1/2 inhibitor) demonstrated a reduction in NF-κB signaling, improvement in bone marrow fibrosis, reduced spleen size, and reduced disease burden.
Myelofibrosis
Myelofibrosis (MF) is one of a collection of progressive blood cancers known as myeloproliferative neoplasms and is associated with significantly reduced quality of life and shortened survival. As the disease progresses, the bone marrow produces fewer red blood cells. The incidences of severe anemia (a condition characterized by low red blood cell counts) and red blood cell transfusion requirements, as well as thrombocytopenia (a condition characterized by low platelet counts in the blood), increase. Among other complications, most patients with MF have enlarged spleens as well as many other physical symptoms, including abdominal discomfort, bone pain, and extreme fatigue.
There are limited treatment options for patients with MF. Ruxolitinib, a JAK1/2 inhibitor, is the current standard of care for intermediate- and high-risk MF patients. Approximately 4-6 per 100,000 Americans are diagnosed myelofibrosis patients (Bose P, Verstovsek S. Myelofibrosis: an update on drug therapy in 2016. Expert Opin Pharmacother. 2016;17(18):2375–2389). Most of these patients are intermediate- or high-risk patients and are therefore eligible for systemic treatment, including ruxolitinib. Many of these eligible patients do not initially receive treatment with ruxolitinib. For example, patients with low red blood cell or platelet counts are ineligible to receive ruxolitinib. In addition, published literature states that up to 75% of patients will have an insufficient response to ruxolitinib within five years of beginning treatment or will not tolerate treatment with ruxolitinib (Verstovsek et al. Journal of Hematology & Oncology (2017) 10:55).
Fedratinib is a second JAK1/2 inhibitor approved for use in treating myelofibrosis. Patients who become refractory to, or discontinue therapy with, ruxolitinib and fedratinib generally have poor survival. Currently approved therapies for treatment of patients suffering from MF offer symptomatic improvement and are generally not considered to be disease modifying.
Pelabresib (CPI-0610)
Pelabresib, also known as CPI-0610, is a potent and selective small molecule designed to promote anti-tumor activity by selectively inhibiting the function of BET proteins to decrease the expression of abnormally expressed genes in cancer. The compound has demonstrated a wide therapeutic window, with activity seen at a 48 mg dose in a lymphoma study and with a maximum tolerated dose of 225 mg. We are using a starting dose of 125 mg in MANIFEST, our global, multicenter, open-label Phase 2 study of pelabresib in patients with MF. Our preclinical studies and translational insights from our first-in-human study of pelabresib led us to prioritize the clinical development of pelabresib in MF.
MANIFEST is testing pelabresib:
- as monotherapy in MF patients who are refractory to or intolerant of, and are no longer on, ruxolitinib (Arm 1);
- as add-on to ruxolitinib in MF patients who have had a suboptimal response to ruxolitinib or have experienced disease progression (Arm 2);
- in combination with ruxolitinib in MF patients who are JAK-inhibitor-naïve (Arm 3)
- as monotherapy in patients with high-risk essential thrombocythemia who are intolerant of, or refractory to, hydroxyurea (Arm 4)
We have also initiated MANIFEST-2, a global, double-blind, randomized Phase 3 clinical study with pelabresib in combination with ruxolitinib versus placebo plus ruxolitinib in JAK-inhibitor-naïve patients with primary myelofibrosis or post-ET or post-PV myelofibrosis who have splenomegaly and symptoms requiring therapy. We are stratifying patients to receive pelabresib + ruxolitinib or the placebo + ruxolitinib. The primary endpoint of the study is a ≥35% reduction in spleen volume (SVR35) from baseline at 24 weeks. A key secondary endpoint of the study is 50% or greater improvement in Total Symptom Score (TSS50) from baseline at 24 weeks. Other endpoints include bone marrow fibrosis grade improvements, duration of transfusion independence, rate of red-blood-cell transfusion for the first 24 weeks, and hemoglobin response.
If you are a US healthcare provider and would like to learn more about MANIFEST-2, click here.
Disclaimer: pelabresib is an investigational medicine and has not been approved by the FDA (or any other regulatory authority). pelabresib is not available for use outside of a clinical trial setting.
EZH2
A Scientific Overview
EZH2 acts as an epigenetic writer and normally places one or more methyl groups on a histone protein, leading to the suppression of gene expression. Some cancers depend on an abnormal pattern of gene expression and re-direct EZH2 to genes that become abnormally repressed. Cancer cells with these abnormal gene expression programs may be more resistant to anti-cancer therapies.
Abnormal EZH2 function has been implicated in a number of ways in specific cancers, a finding that offers broad therapeutic potential for EZH2 inhibition:
- Synergy with oncogenic drivers in prostate cancer
- Activating mutations in lymphoma
- Tumor immunity in solid tumors
- Drug resistance in solid tumors
- Synthetic lethality in genetically defined solid tumors
CPI-0209
CPI-0209 is a second-generation EZH2 inhibitor that has been designed to achieve comprehensive target coverage through extended on-target residence time. The compound has demonstrated more potent anti-tumor activity compared with first-generation EZH2 inhibitors in preclinical models of multiple cancer types. It does not induce its own metabolism, which has been an issue with other EZH2 inhibitors.
We are enrolling patients in a Phase 1/2 clinical trial of CPI-0209. We are dosing patients in the Phase 1 dose escalation portion of the trial. The Phase 1 portion of the trial is evaluating CPI-0209 as a monotherapy in patients with advanced solid tumors. After determining the recommended Phase 2 dose for CPI-0209, which we expect to accomplish in 2021, we intend to pursue expansion arms in selected tumor indications as well as combination therapy development.
Disclaimer: CPI-0209 is an investigational therapy and has not been approved by the FDA (or any other regulatory authority). CPI-0209 is not available for use outside of a clinical trial setting.
LSD1
A Scientific Overview
LSD1, commonly referred to as an epigenetic eraser, removes modifications from chromatin and thereby functions in the regulation of gene expression. Importantly, LSD1 functions in blood cell development, and is required for the maintenance of hematopoietic stem cells as well as for the proper differentiation of erythroid and megakaryocytic cell lineages.
CPI-482
CPI-482 is a potent and selective inhibitor of the LSD1 demethylase enzyme. In the context of MF, we believe that CPI-482 may interfere with the ability of malignant stem cells to replenish the pool of aberrant blood cells. Moreover, CPI-482 may prevent differentiation of megakaryocytes, a cell population that is a key driver of various disease features of MF, including the overproduction of inflammatory cytokines. CPI-482 can also induce differentiation and apoptosis in a number of AML and other cancer cell models and has shown encouraging efficacy in mouse models of hematological cancers. We are currently in IND-enabling studies.
Preclinical Studies
CPI-482 is a potent and selective inhibitor of the LSD1 demethylase enzyme. In the context of MF, we believe that CPI-482 may interfere with the ability of malignant stem cells to replenish the pool of aberrant blood cells. Moreover, CPI-482 may prevent differentiation of megakaryocytes, a cell population that is a key driver of various disease features of MF, including the overproduction of inflammatory cytokines. CPI-482 can also induce differentiation and apoptosis in a number of AML and other cancer cell models and has shown encouraging efficacy in mouse models of hematological cancers. We are currently in IND-enabling studies.
Expanded Access
If you are interested in getting access to a Constellation investigational therapy, please read our Expanded Access Policy, a copy of which may be found here.
All requests will be evaluated in a fair, unbiased manner. If approved, the patient (or his or her guardian) must provide informed consent and consent to comply with the safety and monitoring requirements defined by Constellation.